

Why Skin Punch Biopsies Come Back “Non-Diagnostic” — And How to Improve Your Diagnostic Yield
Few things are more frustrating than submitting a skin biopsy and receiving a report that says:
“Non-diagnostic due to insufficient depth.”
“Extensive necrosis limits interpretation.”
“Inflammation only — no definitive lesion identified.”
When that happens, everyone loses time — and sometimes the opportunity for early diagnosis.
In my experience reviewing surgical pathology submissions, most non-diagnostic skin biopsies are not caused by rare disease. They’re usually the result of small, correctable sampling or handling issues at the time of biopsy.
Here are the most common causes — and how to avoid them.
1️⃣ Inadequate Depth: The Most Common Problem
Many clinically significant processes occur at or below the dermal–subcutaneous interface, including:
Vasculitis
Panniculitis
Deep pyoderma
Early neoplasia
Mast cell tumors
Soft tissue sarcomas
If a punch biopsy stops in mid-dermis, key pathology may be completely missed.
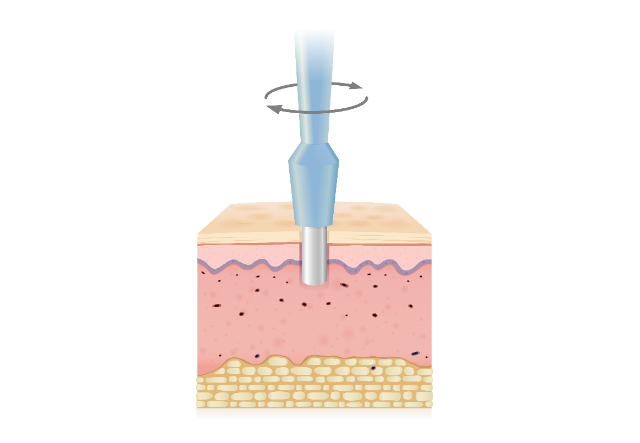
Including subcutis in punch biopsies significantly improves diagnostic yield, particularly for deep inflammatory or neoplastic processes.
Practical Tip:
When performing a punch biopsy, aim to include visible subcutaneous fat at the base of the sample. If you don’t see fat, the biopsy is often not deep enough.
2️⃣ Sampling the Wrong Area of the Lesion
Ulcerated centers and necrotic tissue are common pitfalls.
The center of a lesion may contain:
Secondary inflammation
Necrosis
Granulation tissue
These secondary changes can obscure the primary disease process.
Practical Tip:
For masses, sample the transition zone between normal and abnormal tissue.
For ulcerated lesions, avoid the necrotic center unless necrosis itself is the primary diagnostic question.
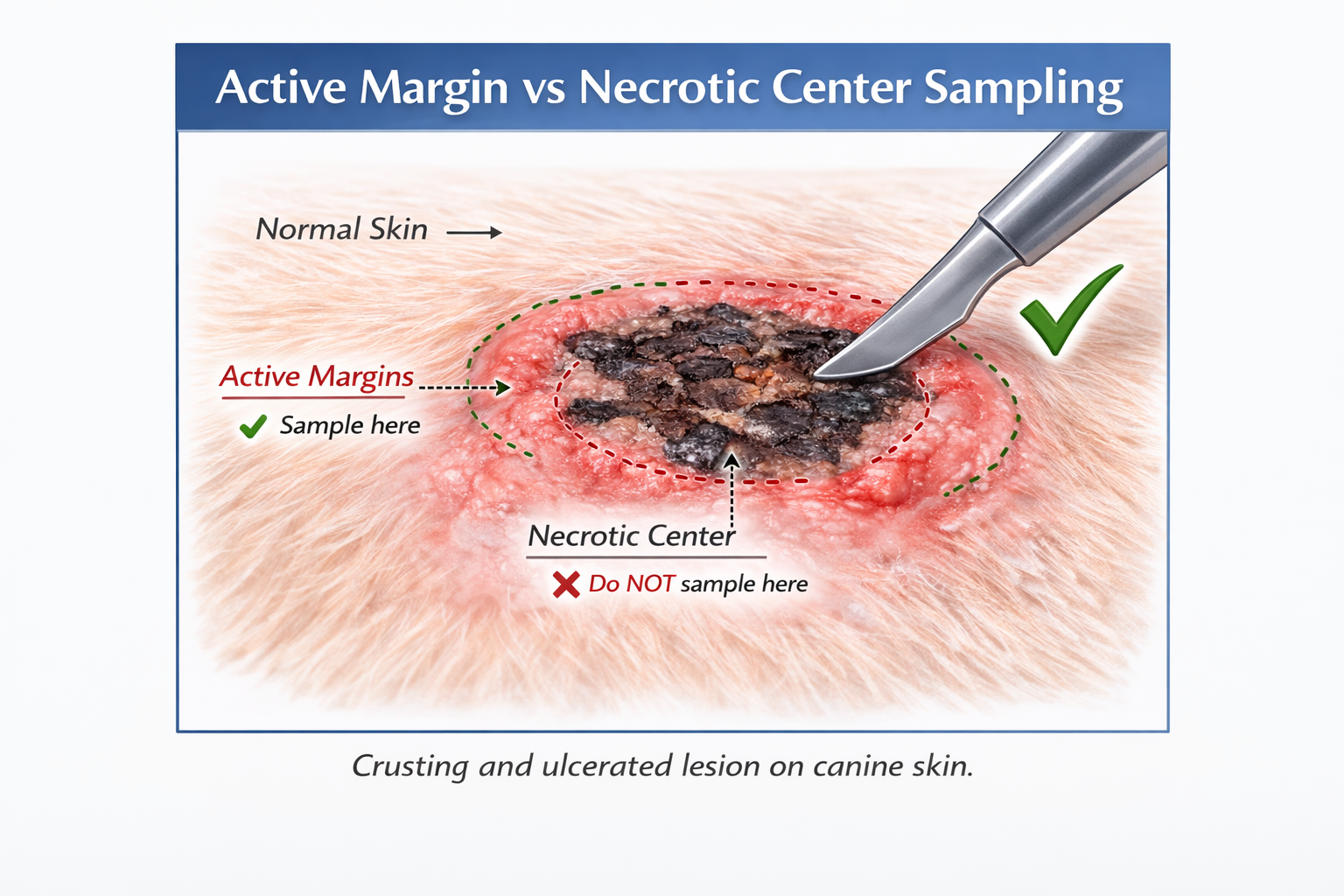
Try not to sample the ulcerated center of a lesion. Collect a sample from the active leading edge. The ulcerated center will have abundant granulation tissue and inflammation as well as potential vasculopathic changes, which may be misleading.
3️⃣ Too Few Samples in Multifocal Disease
Inflammatory and early neoplastic processes can be patchy.
Submitting a single punch biopsy for generalized dermatologic disease significantly reduces diagnostic confidence.
Practical Tip:
For generalized disease, submit 4–6 biopsies from lesions that:
Are not end-stage
Have not been recently treated (if possible)
Represent different morphologies
This simple step markedly improves diagnostic yield.
4️⃣ Fixation and Handling Errors That Compromise Interpretation
Even well-collected biopsies can become difficult to interpret if fixation is inadequate.
Common issues include:
Insufficient formalin volume
Delayed placement in fixative
Storage in saline
Crush artifact from aggressive handling
Freeze artifact during cold weather transport
Practical Fixation Guidelines
Use a minimum 10:1 formalin-to-tissue ratio
Place tissue in formalin immediately after collection
Avoid storing samples in saline
Handle gently — grasp surrounding tissue rather than the lesion core
Avoid squeezing with forceps
Preserving architecture is essential — many diagnoses depend on intact tissue structure.
❄️ Cold Weather Tip: Preventing Freeze Artifact
In freezing temperatures, formalin containers can solidify during transport. Ice crystal formation can distort cellular architecture and create artifacts that complicate interpretation.
To reduce this risk:
Add a small amount of ethanol to formalin when freezing conditions are expected (for example, 1 part 95% ethanol to 9 parts formalin) to lower the freezing point
Use insulated packaging
Avoid leaving samples in vehicles overnight
Schedule pickup to minimize exposure
If freeze exposure is suspected, note this on the submission form — it assists with interpretation.
5️⃣ Clinical History: Lesion Description Makes a Difference
Dermatopathology is highly contextual.
Concise clinical information sharpens interpretation — particularly lesion morphology.
When submitting biopsies, include:
Duration and progression
Distribution (focal, multifocal, generalized)
Pruritus level
Drug history
Previous treatments
Systemic illness
And importantly — a clear morphologic description of the lesion.
Common Morphologic Terms (Brief Definitions)
Macular – Flat discoloration without elevation
Papular – Small, raised, solid lesion (<1 cm)
Plaque – Broad, raised lesion with a flat surface
Nodular – Solid lesion extending deeper into dermis or subcutis
Vesicular – Small, fluid-filled lesion
Pustular – Pus-filled lesion
Ulcerated – Full-thickness epidermal loss
Crusting – Dried serum, blood, or exudate on the surface
Erythematous – Redness due to increased blood flow
Papillary – Finger-like surface projections
Polypoid – Pedunculated or protruding growth
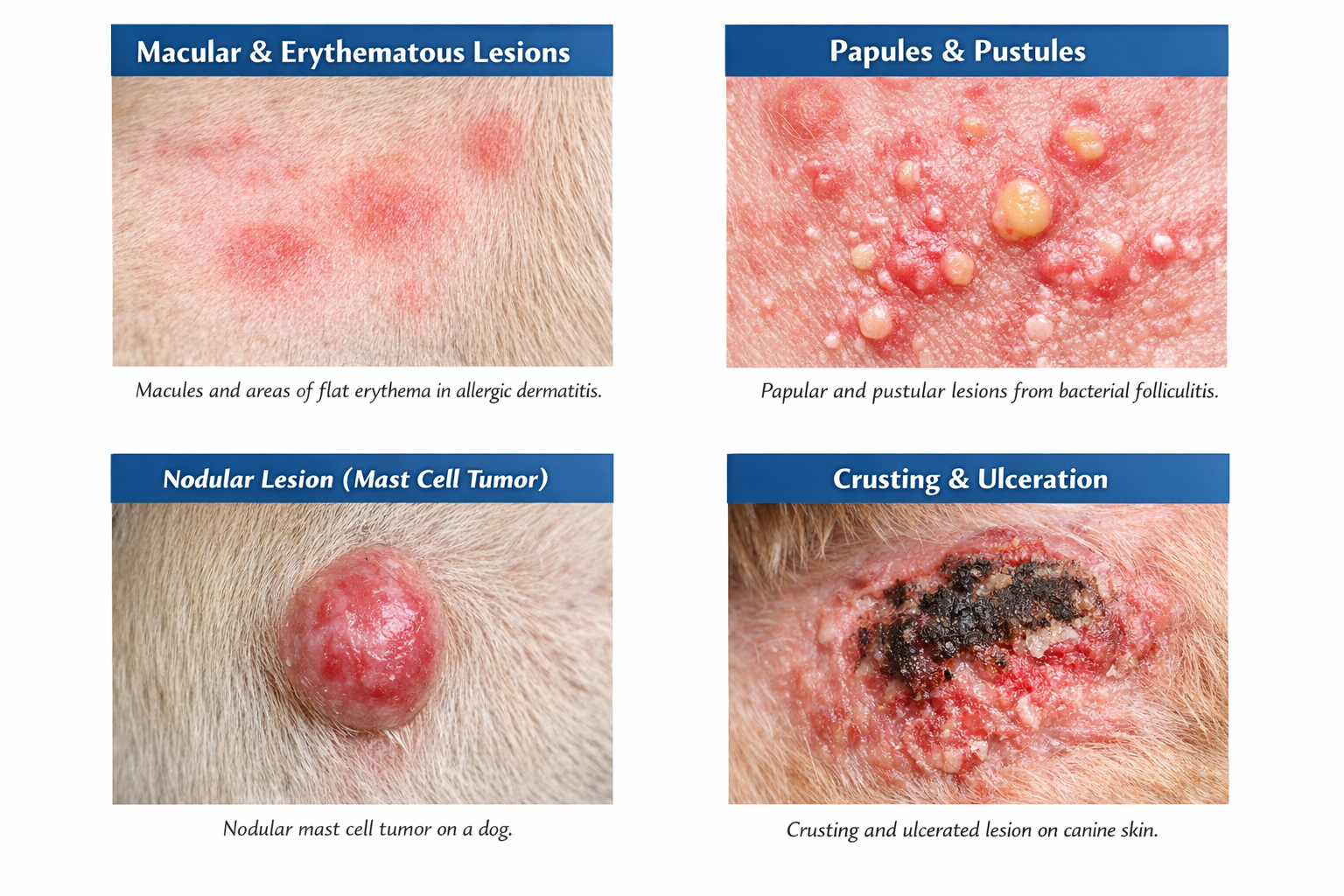
Examples of different types of lesions using descriptions above. Using appropriate descriptions can help the pathologist visualize the lesion more accurately.
These descriptors narrow differentials at the microscopic level. For example:
Papular or pustular lesions often suggest inflammatory or infectious processes.
Nodular or polypoid growths raise stronger concern for neoplasia (or at least proliferative disease).
Ulceration may be secondary — or may reflect aggressive growth.
Four to six well-chosen descriptive lines can meaningfully improve diagnostic specificity.
When to Consider a Wedge or Excisional Biopsy Instead
Punch biopsies are not ideal for:
Large masses
Deep subcutaneous lesions
Rapidly growing tumors
Suspected sarcoma
Margin evaluation
In these situations, an incisional wedge biopsy often provides superior architectural information.
Quick Biopsy Checklist Before Submission
✔ Include subcutis
✔ Sample lesion margins rather than necrotic centers
✔ Submit multiple samples for multifocal disease
✔ Use adequate formalin (10:1 ratio)
✔ Protect specimens during freezing weather
✔ Provide concise history including lesion morphology
Final Thought
Most non-diagnostic skin biopsies are preventable.
If you’re unsure about biopsy strategy for a specific case, I’m always happy to discuss sampling before submission. A brief pre-biopsy conversation can sometimes prevent repeat procedures and improve patient care.